













Neighbors on call: Haiti may offer window to Montana’s healthcare future
Alex Sakariassen / Missoula Independent
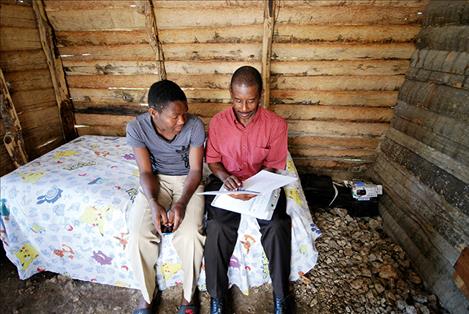
Joseph Benissois, right, queries Presandieu Charles on his mental state during a home visit in June. Benissois has worked as a community health worker in the Haitian town of Cange for more than 30 years.
Keep Reading!
You’ve reached the limit of 3 free articles - but don’t let that stop you.